Minimally
invasive treatment of vertebral compression fractures at Ivy Hospital
by per-cutaneous vertebroplasty by Dr Vineet Saggar
A 54 years old female presented in our OPD with severe pain in back for
past three months. Her X-Ray showed wedge collapse of L1 vertebrae
without canal compromise. She had been on bed rest for three months but
her pain had failed to subside even after full conservative therapy.
She was treated with percutaneous vertebroplasty and her pain was
relieved and she was discharged in fully ambulatory state the next day.
Fig Showing fluoroscopic placement of needle in fractured vertebrae
Fig showing
vertebroplasty cement in fractured vertebrae
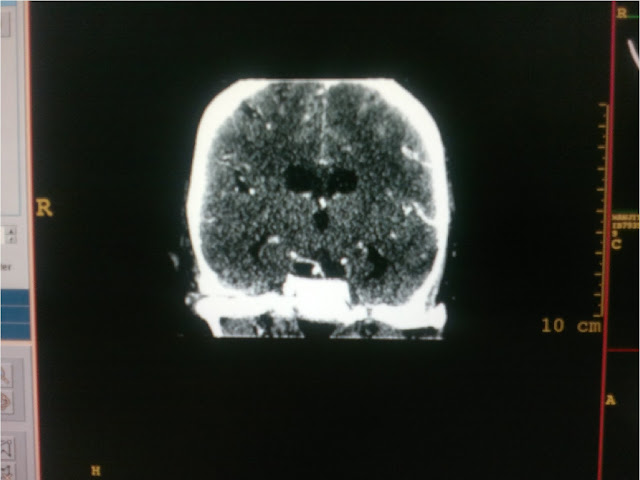
Post Operative Ct scan
showing vertebroplasty cement in L1 Vertebrae
Patient just before discharge
Post op pic showing dressing and small incisions
WHAT IS VERTEBROPLASTY AND KYPHOPLASTY?
This
is a technique of injecting bone cement at the site of painful vertebral
compression fractures under fluroscopyand. Painful vertebral osteoporotic
compression fractures lead to significant morbidity and mortality. A painful osteoporotic vertebral fracture can
be a significant burden for patients (and their families), impairing physical
function and quality of life. Independent of pain, there is morbidity
associated with the spinal deformity. In the thoracic spine this is due to
decreased lung capacity (FVC and FEV1). In the lumbar spine compression
fractures also affect lung capacity, probably due to restrictive airway disease
caused by loss of height, and lead to a reduction in abdominal space associated
with loss of appetite and secondary sequel related to poor nutrition. Additionally,
vertebral body compression fractures (VCFs) cause chronic pain, sleep loss,
decreased mobility, depression, and a loss of independence.
The
medications taken for symptomatic relief can lead to further mood or mental
alterations that compound the medical condition. A large prospective study
noted a 23% increase in mortality in women older than 65 years with VCFs
compared with age-matched controls. The mortality rate increases with the
number of vertebrae fractured. Most painful VCFs are treated palliatively, with
bed rest, narcotic analgesics, orthotics, and time. However, bed rest accelerates
bone loss and leads to muscle de conditioning, resulting in increased pain from
both of these mechanisms. The other
treatments for osteoporosis (e.g., hormone replacement, bisphosphonates,
calcitonin) are important for the long term treatment of this disease but often
do not provide short-term pain relief.
INDICATIONS OF VETEBROPLASTY AND
KYPHOPLASTY
PER CUTANEOUS VERTEBROPLASTY has been used in anterior and posterior
stabilization of the spine for metastatic disease, giant cell tumors of,
treatment of vertebral hemangiomas and . vertebral
compression fractures via the transpedicular or paravertebral approach under CT
and/or fluoroscopic guidance has been described.
TECHNIQUE OF VERTEBROPLASTY AND
KYPHOPLASTY
Upon
completing the informed consent process, the patient is placed in the prone
position on the angiography table. Monitoring of blood pressure, heart rate,
and pulse oximetry is done continuously throughout the procedure. Oxygen
supplied via a nasal cannula is used when necessary. Neuroleptic analgesics in
the form of fentanyl (Sublimaze, Abbott Labs, North Chicago,
Ill) and midazolam (Versed, Roche Pharma,
Manati, Puerto Rico) are administered by the
angiography nurse under the direction of the operating physician. The procedure
is performed under strict sterile conditions. All personnel wear surgical masks
and caps in addition to gowns and gloves for the operators, to minimize the
risk of infection. The vertebral body to be treated is localized under
fluoroscopic control and the skin overlying this area is prepped and draped.
Biplane fluoroscopy
is
recommended, as it allows near simultaneous imaging of the stylet tip position
in two planes, thus decreasing the overall procedure time. The anteroposterior
tube is angled in such a way as to maximize the oval appearance of the pedicle
(“looking down the barrel”) (Fig 1). The skin over the center of the pedicle
oval is anesthetized with bupivacaine hydrochloride (0.25%) followed by
deep injection of bupivacaine to and including the periosteum. A small skin
incision is made with a #11 scalpel blade. A disposable 11-gauge Jamshidi
needle is positioned with Fig 1. The pedicle to be punctured is isolated
and marked with the tip of a surgical clamp. The skin, subcutaneous tissues,
and periosteum are anesthetized with 0.25% bupivacaine. Fig 2. After a small
skin incision is made, the Jamshidi needle is advanced nto the pedicle. Notice
that the shaft of the needle (arrow) maintains a bulls-eye appearance in
relation to the pedicular edges (arrowheads) in the anteroposterior plane. Fig
3. In the lateral plane, the shaft of the needle runs parallel to the
superior and inferior cortices of the pedicle (arrows). After the stylet has
been withdrawn, the needle tip is positioned in the middle of the vertebral
body.

Figure 1 Figure 2 Figure 3
its tip in the center of the oval and
advanced until the stylet tip abuts the bone. Lateral fluoroscopy shows the tip
at the level of the upper to midpoint of the pedicle such that advancement of
the needle is within the midportion of theof
the pedicle oval to indicate that the needle is proceeding parallel to
the X-ray beam (Fig 2). The lateral view shows the needle moving roughly
parallel to the superior and inferior edges of the pedicle (Fig 3) or
in a slightly descending course through the pedicle. Minor
adjustments in either plane may be required during needle advancement.
Once the needle tip has traversed the cortex and the pedicle. A slight twisting
motion is used to advance the tip through the cortex, and frequent checking of
needle placement in both planes is required. The anteroposterior view shows the
needle shaft end-on as a circle within the center
pedicle and is located within soft bone marrow, less pressure may be required
to advance the needle into the vertebral body. Care must be taken not to
abrogate the anterior vertebral wall or the endplates. The stylet tip is placed
at or near the junction of the anterior and middle third of the vertebral body
line. Because the stylet tip projects beyond the end of the needle shaft,
removal of the stylet will position the needle end in the middle or
anterior half of the vertebral body (Fig 3). Before injecting the PMMA,
venography is done to exclude needle placement directly within the
basivertebral venous complex and to ensure continuity of the posterior
vertebral wall as evidenced by containment of the contrast material within the
bony trabeculae (Fig 4). We use a hand injection of 5 mL of iohexol (Omnipaque
300, Nycomed,Princeton, NJ) and film in both planes at a rate of two
frames per second. Rapid flow of contrast material into the vena cava and/or
perivertebral veins without visibility of intervening bone marrow indicates
direct communication of the needle tip with a major venous outlet and requires
needle advancement. Once correct placement of the needle is confirmed,
treatment is begun. If a bone biopsy is warranted, a variety of standard,
commercially available biopsy needles can be passed through the Jamshidi shaft
to obtain tissue samples before vertebroplasty One operator injects the
material as the second loads the syringes. The stylet is removed and,
unless blood fills the dead space in a retrograde manner, the dead space is
injected with PMMA using a long 18-gauge spinal needle. The 1-mL syringe is
attached tightly to the shaft port of the Jamshidi needle and injection begins.
The injection pressure required to push the material will increase over time
as the vertebral body fills and the PMMA polymerizes. Injection is performed
under lateral or anteroposterior oblique fluoroscopy ( and particular attention
must be paid to the region of the vena cava and the epidural space as seen on
the venogram. If passage of material into the venous system is when
appropriate.noted, the injection is slowed or halted while the material attains
a thicker consistency. Injection is continued until hemivertebral or
holovertebral filling is achieved, no more material can be pushed into the
body, or extravasation into veins or the disk space is noted. Repositioning of
the needle is not recommended, as the location of the tip will be unknown, and
unwanted vascular embolization may occur. Upon completing the injection,
the needle is removed and hemostasis at the puncture site is achieved by gentle
pressure. The contralateral hemivertebra is then treated in the same fashion.
More than one vertebra can be treated at the same time, depending on the
patient’s tolerance After the procedure, the patient is placed supine and
asked to remain flat for 3 hours to allow complete curing of the PMMA prior to
axial loading. Although patients usually remain overnight, those from our local
area are allowed to return home the same day.
Dr. Vineet Saggar (MCh)
Neuro Surgeon / Spinal Surgeon
Chandigarh, Mohali -
Ivy Hospital Sector 71
+91-9855990990
http://www.slideshare.net/neurosergeonhead